

Editorial Note: This brief was updated on September 17, 2025 to reflect language in the final bill enacted July 4, 2025.
On July 4, President Trump signed into law the budget reconciliation bill, previously known as “One Big Beautiful Bill Act.” The law includes several policy changes that could have significant implications for the health and health coverage of older Americans ages 50 and older, including those who are covered by Medicare.
The reconciliation law as enacted includes an estimated $911 billion in federal Medicaid spending cuts over the next 10 years, including several provisions expected to increase costs or eliminate coverage for Medicaid beneficiaries. Collectively, these provisions could affect the 22 million people ages 50 and older with coverage under the Medicaid program by reducing the number of people with Medicaid and reducing access to health and long-term care services for people who remain enrolled in the program. The reconciliation bill also includes changes that are expected to reduce the number of people with ACA Marketplace coverage, including among individuals between the ages of 50 and 64.
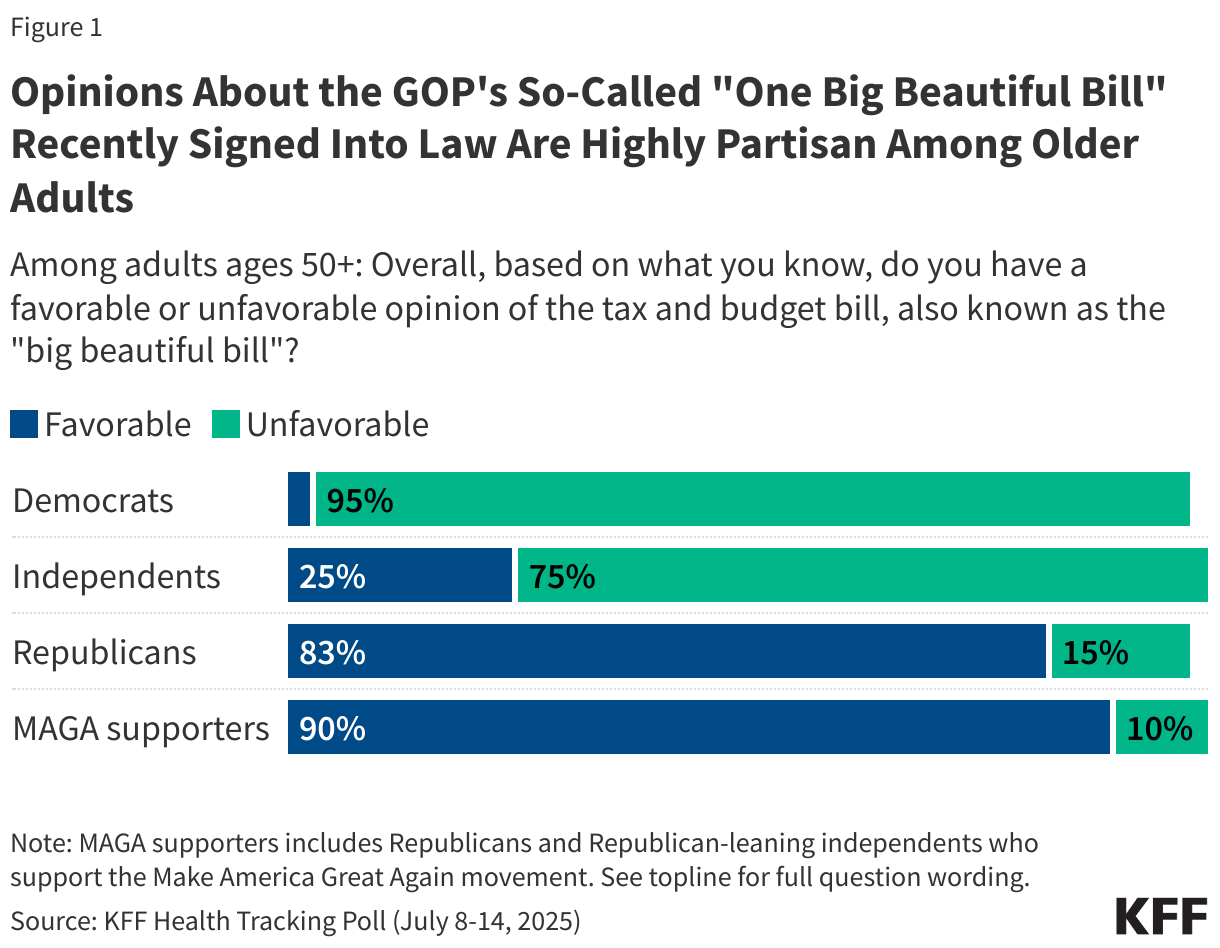
According to KFF’s Health Tracking Poll conducted in July of 2025 less than half (42%) of older adults have a favorable view of the just-passed tax and budget law, including 39% of people ages 50-64 and 44% of adults ages 65 and older, with far stronger support among older adults who are Republicans (83%) than those who are independents (25%) or Democrats (3%). (See Figure 1 below).
Below are seven health-related provisions to watch as provisions of the 2025 budget reconciliation law are implemented.
1. New Medicaid Work Requirements. The largest source of federal Medicaid spending cuts will come from new work requirements that will be imposed on the Medicaid expansion population. The Congressional Budget Office (CBO) estimates that the work requirements would reduce Medicaid spending by $326 billion and cause nearly 5 million people to become uninsured.
The new law requires adults ages 50-64 to meet new work and reporting requirements if they are enrolled through the ACA expansion. Most Medicaid enrollees ages 50-64 are working or could be exempt from the work requirements because of a disability or caregiving responsibility, but they will still need to comply with reporting requirements, putting them at risk of risk losing Medicaid coverage. According to a new KFF analysis, fewer than half of adults ages 50-64 would meet the work requirements through either employment or school, compared with 72% of adults ages 19-27 and 66% of adults ages 27-49.
2. Changes to ACA Marketplaces. An estimated 5.5 million adults ages 55 to 64 get health insurance from ACA Marketplaces in 2025. The law makes changes to the ACA Marketplaces that will increase the number of people who are uninsured, including older people ages 50-64. Combined with the Trump administration Marketplace integrity rules, the law will shorten the open enrollment period, impose new documentation and pre-enrollment verification of eligibility requirements, and make other changes that would affect enrollment. Overall, the outcome will be loss of health insurance coverage for as many as 3 million people by 2034, including older adults.
Further, because the law does not extend enhanced ACA premium tax credits for Marketplace coverage that are set to expire at the end of 2025, an additional 4.2 million people (including older adults) are estimated to lose coverage by 2034. Without enhanced premium tax credits, Marketplace enrollees with incomes over four times poverty will lose subsidy eligibility and those with incomes between 100% and 400% of poverty will receive a smaller tax credit.
Over half of individual market enrollees with incomes above four-times the poverty threshold are between the ages of 50 and 64, which means that older adults will be disproportionately affected if the premium tax credits are not extended beyond this year. Furthermore, the loss of premium tax credits for those over 400% of poverty means that group will bear the full cost of any premium increases on top of the loss of financial assistance. Premiums are expected to increase by about 18% in 2026.
Health insurance premiums are higher for people in their 50s and early 60s than for younger adults choosing the same plan in the same area. If the enhanced premium tax credits expire, Marketplace enrollees currently receiving a subsidy could face higher costs to enroll, particularly if their incomes are about or above 400% of poverty. For example, according to the KFF calculator, a 59-year-old single widow living in Jackson, Missouri earning $63,000 (just above 400% of the poverty level) would pay $5,355 for her silver Marketplace plan in 2026 if Congress acts to extend the enhanced premium tax credits before the end of this year. But if Congress does not extend the enhanced premium tax credits, she could pay more than twice the amount—$14,213 in premiums a year—or 22.9% of her income for the same health insurance policy. It’s not hard to see why she and others like her might give up their Marketplace plans, given the cost relative to their income.
3. Placing a Moratorium on Implementation of the Medicare Savings Program and Medicaid Eligibility and Enrollment Rules. Older adults are also at risk of losing coverage due to provisions in the law that impose a moratorium on implementation of most provisions in two Biden-era rules that were intended to streamline the enrollment process for Medicaid, especially for older adults and people with disabilities. The fourth largest source of federal reductions in Medicaid spending stems from these two provisions, which are collectively estimated to reduce federal Medicaid spending by $122 billion.
Both rules aimed to reduce barriers to enrolling in and maintaining Medicaid coverage. They were expected to disproportionately affect enrollment among older adults and people with disabilities because they included specific requirements related to streamlining Medicaid enrollment among Medicare beneficiaries, and to facilitating smoother enrollment for people who are eligible for Medicaid because they have a disability, are ages 65 and older, or use long-term care.
Earlier CBO analysis showed that delaying implementation of these rules would mean that 1.3 million fewer Medicare beneficiaries would also have Medicaid coverage in 2034. That number may be lower under the law as enacted based on the Senate’s changes to the legislation, because CBO’s estimates of the savings associated with the provisions decreased from $167 billion prior to those changes to $122 billion for the law as enacted. A separate KFF analysis shows that the loss of these Medicaid benefits would result in a someone with an income of $967 per month paying $185 per month in Medicare premiums, or about 20% of income, without accounting for other non-trivial out-of-pocket costs, including Medicare cost-sharing requirements and the loss of Medicaid benefits.
4. Reducing Spending for Long-Term Care Services.The reconciliation law could also reduce federal funds for nursing facilities and would likely lead to reductions in spending for other long-term care services. The law will reduce federal Medicaid spending by $23 billion over 10 years by prohibiting implementation of a Biden Administration rule on nursing facility staffing. The rule had aimed to help address long-standing concerns about inadequate staffing and the quality of care, but the law locks into place a federal judge’s ruling to overturn key elements of the rule.
The reconciliation law could also reduce Medicaid funds available to nursing facilities through a moratorium on provider taxes (in place for nursing facilities in 46 states) and new limits on some payments to nursing facilities (known as state-directed payments). Savings from provisions affecting provider taxes and state-directed payments account for $340 billion in reduced federal Medicaid spending over 10 years, although they would also affect hospitals and other providers. KFF estimates that at least 29 states would have to reduce existing state-directed payments to hospitals or nursing facilities under the enacted legislation.
If experience from the past is a guide, substantial cuts to federal Medicaid spending could lead to reduced spending on home care, which includes long-term care provided in people’s homes and the community (and is sometimes referred to as home- and community-based services or HCBS). During the last major reduction in federal spending, all states reduced spending on home care by serving fewer people (40 states) or by benefits or cutting payment rates (for long-term care providers) (47 states). As a significant source of Medicaid spending comprised of optional services for which there are already waiting lists, home care may be especially vulnerable.
5. Ending Medicare Eligibility for Previously Eligible People with Lawful Immigrant Status. Under current law, undocumented immigrants are not eligible for Medicare. Medicare coverage is restricted to people who are citizens or permanent legal residents. The 2025 budget reconciliation law prevents defined groups of individuals who are lawfully present in the U.S. from becoming eligible for Medicare benefits and terminates Medicare coverage for currently eligible beneficiaries who are not U.S. citizens, green card holders, certain Cuban-Haitian entrants, and people residing under the Compacts of Free Association no less than 18 months from enactment. Individuals affected by this provision and their employers would continue to be required to pay Medicare payroll taxes. This is the first time that Congress has eliminated Medicare coverage from previously eligible legally residing individuals. According to CBO, the provision will save $5.1 billion over 10 years, and result in 0.1 million Medicare beneficiaries losing their Medicare coverage as of 2034.
6. Adding Work Requirements and Cutting Federal Spending for Supplemental Nutritional Assistance Program (SNAP). The reconciliation law reduces federal spending for SNAP by about $186 billion. Reductions of this magnitude, coupled with work requirements, are likely to affect the health of older adults, particularly given the strong ties between health and nutrition. As noted above, work requirements, even with exemptions, pose administrative hurdles for older adults that put them at risk for losing SNAP benefits. An estimated 9.2 million Medicare beneficiaries received SNAP benefits to help cover the costs of food and groceries in 2022, according to a KFF analysis. The SNAP work requirements may particularly exacerbate financial challenges for older Medicaid enrollees ages 50 and older who are two and a half times more likely to experience food insecurity than other older adults not enrolled in Medicaid (28% compared to 10%).
7. Modifying the Medicare Drug Price Negotiation Program to Delay or Exempt Certain High-Spending Drugs from Negotiation. Under the Medicare Drug Price Negotiation Program, the federal government is required to negotiate with drug companies for the price of some high-spending drugs that have been on the market for several years without competition, with the goal of lowering Medicare drug spending and helping to reduce out-of-pocket costs for people with Medicare. The law that created the negotiation program exempted drugs from negotiation if they were designated and approved for only one rare disease or condition (known as orphan drugs).
The reconciliation law exempts orphan drugs from Medicare drug price negotiation if they are approved for two or more rare diseases or conditions, not just a single rare disease. It also delays the timeframe for Medicare price negotiations for orphan drugs that are subsequently approved for non-orphan indications. These changes have the effect of delaying the negotiating process for some drugs, while exempting others from negotiations altogether, which is projected to diminish savings to Medicare from the negotiation program.
The changes are expected to have an immediate impact on which drugs are selected for Medicare price negotiation in 2026, including, for example, likely delaying the selection of the cancer drug Keytruda by a year. In 2023, Medicare and the 70,000 beneficiaries who used Keytruda spent a total of $5.6 billion on this drug alone, with annual out-of-pocket liability averaging around $15,000. By exempting or delaying price negotiation for Keytruda and other orphan drugs, the reconciliation law is likely to lead to higher out-of-pocket costs for beneficiaries who take these drugs relative to what they would have paid if a lower, Medicare-negotiated price was available.
This work was supported in part by the John A. Hartford Foundation. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.